



States and Cities Need to Protect Our Health, Because the Feds Won’t
Some have leadership thrust upon them
(I drafted this to submit as an op-ed, but it’s too urgent for that, so here goes.)
The shutdown of the MMWR. The attempt to stop federal grants. The federal worker buyout memo. If the Trumpians wanted to shock us, they have succeeded.
Which means that maybe their handling of public health won’t be as bad as we expected. It will be much worse.
With Trump’s picks to lead CDC and HHS, we expected political meddling and hostility at the top. But now it seems we may be headed for a complete decapitation of leadership on public health. That ought to scare everyone, because this nation won’t go four years without a health crisis erupting.
We’ve had plenty of warnings that bird flu could become the new COVID-19. And history teaches us to also expect unknown unknowns – like a new disease (HIV/AIDS), an old disease that has found new ways to spread (Mpox), a malicious act (anthrax) or a toxic substance that has been unleashed (the epidemic of lung disease called EVALI).
If CDC is neutered, untrustworthy, or a hollow shell, state and local health departments will have to step up to protect our health – quickly. Most aren’t prepared.
State and local health departments – the arms and legs of the national public health system - do far more than most people recognize. They keep a lid on diseases like measles and whooping cough by enforcing requirements that children be vaccinated to enter school. They prevent outbreaks of salmonella by inspecting restaurants. They keep our tap water safe by testing water systems. They help pregnant women find prenatal care and keep persons with tuberculosis on treatment to prevent the disease’s spread to others. When a dozen people get dysentery after a church social or a cluster of seniors in a nursing home contracts pneumonia, it is staff from the state and local health departments who are first on the scene.
But behind these state and local health departments stands the CDC, full of experts on every disease of public health importance. CDC’s epidemiologists and lab scientists are the world’s best at investigating epidemics, figuring out what is causing them, and issuing guidance on how to end them. When a strange type of pneumonia sickened hundreds of men attending a convention of the American Legion in Philadelphia in 1976, it was the CDC’s scientists who identified the previously-unknown bacteria that caused it, and it is the CDC today that still prevents repeats of that outbreak through advice on how to maintain air conditioning and water systems. It is likewise CDC’s guidance that doctors, hospitals, schools, employers, and many other organizations nationwide follow to prevent the spread of other infections, from measles to parasites in our water systems.
As of last week, CDC also sent some $7 billion in grants to state and local health departments, without which they would have trouble running prevention programs. That money pays for epidemiologists, laboratory equipment, and staff to limit the spread of sexually transmitted diseases and tuberculosis, for example. It’s this type of funding that has helped HIV/AIDS shrink from a national crisis to a manageable problem.
Unfortunately, that strength of CDC has, over years, fostered a complementary weakness among state and local health departments. Too often the leaders of these departments, instead of being public health experts, are chosen by governors and mayors to placate a constituency or return a favor – a friend of a friend who has an MD and is unlikely to stir up trouble.
Below those leaders, the infrastructure of most state and local health departments is weak. These departments don’t have the specialized laboratory equipment or skilled staff needed to identify new or emerging infectious agents. They don’t have large teams that can be mobilized to conduct major outbreak investigations. They aren’t staffed with experts who can write guidance needed by others. They don’t have ground troops that contain outbreaks by holding mass clinics to distribute vaccines or antibiotics. And they aren’t equipped to take the lead in fighting what are in fact the biggest killers today, chronic diseases like heart disease, cancer, chronic lung disease, and diabetes.
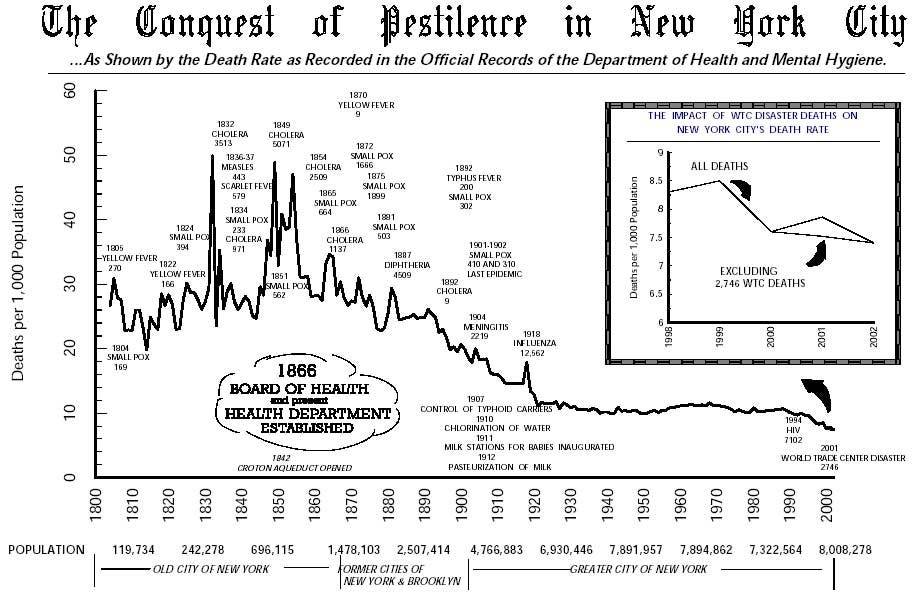
It wasn’t always like this. The CDC was established only in the 1940s, originally just to fight malaria. Before then, health departments in states and big cities led the battles against the health threats of the day. The most prominent doctors ran health departments. State and local “sanitary commissions” investigated health problems and made sweeping recommendations that became enacted into laws. It was the New York City health department that in 1897 took the lead in controlling tuberculosis by requiring physicians report every case they diagnosed, and then isolating people with TB during treatment. In the 1890s, the New York City health department even manufactured its own diphtheria vaccine and administered it for free to the poor, cutting death rates from diphtheria in half. But as with other government functions, over the past century, legal authority, money, and power in public health has migrated from states to the federal government.
Occasionally, local health departments still take national leadership on specific issues. In the Bloomberg years, the New York City health department combatted chronic diseases by making bars and restaurants smoke-free, banning trans fat, and requiring restaurants to post calorie counts. Opponents at the time called these actions overreach, but the policies spread nationwide. In 2017-18, the health departments in Philadelphia, Oakland, Seattle, and San Francisco worked with advocates to pass taxes on sugary drinks to slow the obesity epidemic. But these examples are more the exception than the rule.
In the absence of trusted national leadership, state and local health departments must build the strengths that they don’t now have. They need to hire subject-matter experts who can speak with authority, people to analyze data, and staff to write guidance documents. They will need teams who can not only investigate outbreaks but also contain them – including and especially outbreaks that are massive COVID-19-like events. They may need to write their own weekly newsletters to keep health care providers abreast of emerging health threats. They will need to strengthen their own legal authority and regulatory capacity to shut down sources of disease and get dangerous consumer products off store shelves.
What do state and local health departments need to grow into their roles? First, money. The CDC grants to prevent infectious diseases or chronic diseases may end. Second, people. They’ll need epidemiologists, laboratory scientists, inspectors, community workers who can operate pop-up clinics, and more. Those people exist, particularly because many current CDC workers will soon be looking for jobs. But to hire them, state and local health departments will need flexibility from rule-bound Civil Service systems that can’t handle people with special skills.
Most important, state and local health leaders, with the support of their governors and mayors, must undergo an attitude shift. They must see themselves as not just the arms and legs of public health, but also the brains. They must become leaders in the true sense, who make their own decisions about how to protect the health of their constituents, rather than look to CDC for direction. Starting last week, the buck stops with them.
Thanks for using 2 words to destroy the careers of hundreds of CDC-ers struggling on the job market.
This is right on. Some things can't be privatized, and prevention is one of them.